



Impact of Antihypertensive Drug Selection on Mortality and Heart Disease in Elderly Patients
Introduction
Hypertension is a prevalent condition among the elderly, particularly those aged 75 and older. It is a major contributor to cardiovascular diseases and mortality. As Japan experiences rapid aging, effectively managing hypertension has become increasingly critical. Recent studies have demonstrated that while antihypertensive medications have been widely evaluated across various age groups, high-quality direct comparison evidence for first-line treatments specifically for those aged 75 and above has been lacking.
Research Background
Most elderly patients often contend with multiple chronic illnesses, making it challenging to conduct randomized clinical trials that effectively evaluate the efficacy of antihypertensive drugs in this demographic. Angiotensin receptor blockers (ARBs) and calcium channel blockers (CCBs) are the primary antihypertensive medications prescribed in Japan. While both drugs successfully lower blood pressure, their differing mechanisms may lead to varied clinical outcomes—an important consideration as the physiological changes associated with aging could influence overall health.
Methodology and Findings
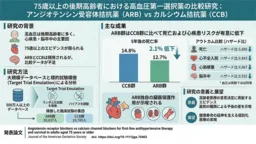
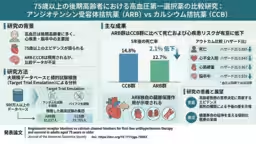
A research team led by Professors Hisashi Noma and Haruhisa Fukuda analyzed data from over 5 million patients collected in a national comprehensive database known as the LIFE Study. Utilizing a modern data science method called target trial emulation, they generated results mimicking a randomized clinical trial. Their analysis involved a cohort of 29,822 patients—divided into groups receiving either ARBs or CCBs.
The findings were compelling:
- - The ARB group exhibited a significantly lower risk of mortality (Hazard Ratio 0.885, 95% CI 0.823-0.951) compared to the CCB group.
- - After five years, mortality rates recorded were:
- CCB Group: 14.8% (indicating a 2.1% absolute risk reduction in ARB patients).
- - Additionally, the ARB group showed reduced risks for several adverse events:
- Myocardial infarction: HR 0.867 (95% CI 0.795-0.945)
- Stroke: HR 0.931 (95% CI 0.869-0.998)
- End-stage renal disease/Dialysis: HR 0.611 (95% CI 0.354-1.056)
The blood pressure levels maintained during treatment were nearly identical in both groups, suggesting that the beneficial outcomes attributed to ARBs likely extend beyond mere blood pressure reduction, hinting at intrinsic organ protective properties of the drug.
The Significance of the Research
For the first time, this study provides substantial evidence linking the type of antihypertensive medication chosen to survival rates and heart failure outcomes in elderly patients. With Japan's swift demographic shifts, establishing this scientific groundwork is crucial. The implications of preferring ARBs over CCBs suggest that the properties of ARBs might specifically address risks that accrue with aging, offering better management strategies for cardiovascular health in older adults.
Future Directions
This research equips healthcare providers with valuable insights when prescribing antihypertensive agents to patients aged 75 and older. Future investigations will focus on analyzing the broader impacts of these medications on frailty, patient autonomy in daily living, and long-term kidney function effects. Building detailed, context-appropriate evidence is necessary to refine clinical guidelines and contribute to a healthcare paradigm that emphasizes longevity alongside improved health span, ultimately enhancing quality of life for an aging population.
Conclusion
The findings from this research mark a pivotal shift in understanding how medication choices can directly influence health outcomes among the elderly. As the global population ages, these insights will serve as a cornerstone for personalized medicine approaches aimed at fostering not just longevity but healthy aging.
References
- - Noma, H., Fukuda, H. et al. "Angiotensin receptor blockers vs calcium channel blockers for first-line antihypertensive therapy and survival in adults aged 75 years or older." Journal of the American Geriatrics Society, DOI:10.1111/jgs.70463.


Topics Health)
【About Using Articles】
You can freely use the title and article content by linking to the page where the article is posted.
※ Images cannot be used.
【About Links】
Links are free to use.